
“To build a sustainable infrastructure for monitoring, tracking, and reporting diabetes data at the local level.”
The goal of Western Tribal Diabetes Project (WTDP) is to provide technical assistance to Northwest Tribes to develop a system for sustained data collection, reporting, and utilization. The objectives of WTDP are designed to assist the Tribes:
Build a foundation to provide complete and accurate information about patients with diabetes
Estimate the burden of disease and impact of diabetes by using an electronic diabetes register
Improve health outcomes by using an electronic diabetes register to make informed decisions about clinical diabetes care
Prevent diabetes in high-risk individuals.
WTDP has developed several tools to guide diabetes programs through a step-by-step approach for data improvement and health promotion. To learn more about WTDP, including our step-by-step approach and tools, please visit our Project Information Page.
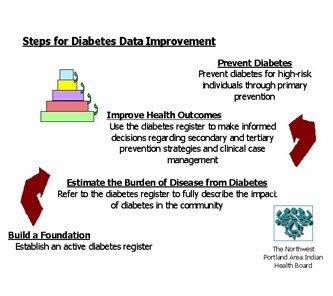
- Build a Foundation This step involves establishing an active, accurate diabetes register. Activities in this step include developing a work plan, conducting medical chart reviews, and establishing a diabetes team.
- Estimate the Burden of Disease from Diabetes During this step the diabetes register is used to fully describe the impact of diabetes in the community. Activities include estimating the prevalence of diabetes, performing and reviewing the IHS Diabetes Audit, and estimating the incidence of complications.
- Improve Health Outcomes This step involves using the diabetes register to make informed decisions regarding prevention strategies and clinical case management. Activities including working to prevent complications in existing patients living with diabetes, improving clinical case management, and shaping program planning.
- Prevent Diabetes At this step the goal is to prevent diabetes for high-risk individuals through primary prevention. This step initiates a new cycle of steps: building a foundation for prevention, estimating the burden risk for diabetes, and improving health outcomes.













